Symptoms of PLC damage
Patients who have chronic deficiency of the one or more structures of the PLC may complain of:
- Pain in this area of the knee joint, or in the medial (inside) area of the knee joint
- Hyperextension of the knee during walking, where the knee feels like it is going backwards
- Varus, or bowed leg, which is very noticeable during walking and jogging – especially compared to the opposite leg which is normal
- Feelings of instability, or actual giving-way, during sports or daily activities (sometimes with activities as simple as walking)
- A failed ACL or PCL reconstruction
- Severe atrophy (wasting) of the quadriceps muscle and other muscles in the leg and hip
Untreated deficiency of the PLC is one of the most common causes of failure of cruciate ligament reconstructions. Studies at our Center documented this finding in 30% of patients referred to us with a failed ACL reconstruction. In most of these patients, the PLC damage was not diagnosed and therefore, not treated.

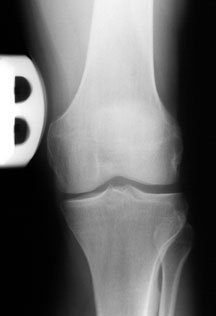
As you will learn, deficiency of the PLC causes an abnormal increase in the amount of joint space between the femur and tibia on the lateral (outer) part of the knee. This is termed abnormal lateral joint opening – and this places harmful forces on a healing ACL or PCL graft that eventually causes the graft to fail.
This is clearly evident in the x-ray on the left as shown by the yellow arrow – compared to the normal, uninjured knee on the right. [The white things are the metal fixations put in during the operation.]
Patients with severe untreated deficiency to the PLC have tremendous disability with normal daily activities, are not able to walk normally, and have constant pain. The reasons for this are all of the abnormal motions that occur in the knee which technically are:
We will talk about these abnormal motions in everyday language later in this course.
It is important to note from the very beginning that there have been many operations described to reconstruct deficient or torn PLC structures. Unfortunately, not all of these procedures have good success rates. Recently, there has been a trend towards what is called an “anatomic” reconstruction in which high strength grafts are placed in the exact location of the deficient ligaments and soft tissues. These procedures have excellent (short-term) results and are now recommended by surgeons experienced with this problem.
Next, we will tackle the anatomy and terminology of the posterolateral region of the knee joint and briefly explain why these structures are important for stability.
COURSE INTRODUCTION: Posterolateral corner injuries of the knee - course