The second key point is the link between movement, applied force, stretch and deformation, and perturbation of noxious nerves contained within the fat pad.
This pattern of non-isometric mechanical behavior stretch and distortion of the ligamentous IPP and fat pad is confirmed in the kinematic videos and in Figures 5 and 6 which consists of screen shots from the fluoroscopies of volunteers in the In-Vivo study. Because the fat pad is tethered centrally by the IPP and to its wide fibrous attachment on its periphery, it is held captive within the borders of the anterior compartment.

Our studies, and those of others demonstrate that the fat pad is highly innervated, its nerves either protected in lobular fat or coursing within the elastic septa. The central body transition zone contains a network of neurovascular bundles lodged and also protected in the lobular fat between finger-like dense connective tissue bands that merge to become the rope-like central zone of the IPP. There are also sparse nerves in the plica itself. An orthopaedic surgeon, Scott Dye, heroically demonstrated the synovial membrane, lining the entire joint, is moderately to severely painful to physical pressure, and that the most sensitive tissues of all are the fat pad and immediately adjacent structures (ref. 3).
The basic structure of the fat pad is thus a fibrous scaffold (ref. 4), packed with lobules of compressible fat, highly innervated throughout. On its periphery anteriorly the fat pad is then widely and firmly attached to the fibrous capsule and patellar tendon. It is tethered centrally by the IPP which is, as we have confirmed, a non-isometric ligament (ref. 1). The anterior compartment borders are bony and cartilagenous on 3 sides and firm fibrous capsule and ligament in front. As the knee moves, the geometrically complex borders constantly change. Tethered by the IPP between, the fat pad must stretch, relax and deform with knee motion. If the contained noxious nerves have been activated to a painful state by some pathology in the knee, the patient will perceive added pain related to this physical perturbation of these nerves.
Forces applied to and through the anterior compartment are seamlessly transmitted with appropriate attenuation through the IPP-fat pad complex to the apex of the notch via the central body and IPP, and to the tibia via the inferior dense connective tissue (DCT) bands.
We were able to demonstrate effect of these connections in vivo in the volunteer study by asking the patients to do a “quads set” manouevre, maximally contracting the quads with the knee locked in full extension. The patella moves about a centimeter as the 18-year-old volunteer “gets it” contracting forcefully her quadriceps in knee-locked position.
Untethering of the fat pad
Once untethered by release and resection of the IPP the kinematic videos confirm that the untethered fat pad shows virtually no stretch and distortion. This correlates with absolute pain relief. With motion eliminated in the quads set, it is the connective tissue links in the synovial layer, the alar folds, and the superior dense connective tissue bands that transmit these forces.
In Figure 9 below, the fat pad fills the anterior compartment, its contour matching the curves of the condyles and occupying the notch, as well, in full flexion. Virtually all of the deformation and stretch of the IPP-fat pad complex has been eliminated. The radiograph represents gross anatomy. These videos thus provide radiographic correlation between the clinical problem of AKP and the structure of the IPP-fat pad complex. Untethering the fat pad allows it simply to fill the anterior compartment without painful eccentric distortion and stretch.
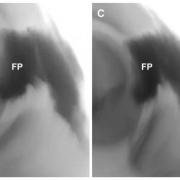
Figure 10. Kinematics of the IPP-FP complex after release of the IPP; screenshots from Video 2. The cyclical stretch, and relaxation of the IPP, plus the distortion and stretch of the central body and fat pad has been abolished by release of the IPP at the femoral attachment. The fat pad fills the available space without the distortion visible when the IPP is present. The IPP and femoral attachment are simply not seen post release and partial resection.




