I am going to leave you to familiarise yourself with the relevant anatomy, and the links in the text as well as the keyword tags at the top of this page will help you to find this information.
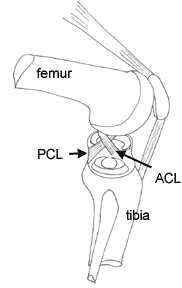
It is important to understand the relationship of the cruciate ligaments to one another, and also to appreciate their attachments in the flat upper surface of the tibia and in the intercondylar notch. For instance, the ACL attachment is located on the lateral femoral sidewall of the notch; no ACL fibers extend to the intercondylar roof. ACL grafts which are placed in the "roof" of the intercondylar notch are vertical in orientation, unlike the native ACL, and are therefore prone to failure. The important anatomic positioning means that any graft has to be placed with great precision that replicates where the original ligament was located. (The illustration shows the structures of the right knee from the side. PCL=posterior cruciate ligament).
Collateral ligaments, menisci and meniscal ligaments
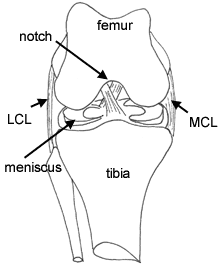
The menisci act as spacers and shock absorbers, cushioning the impact between the rounded ends (condyles) of the femur and the flattened end (plateau) of the tibia. They also play a role in knee stability, with the medial meniscus intimately related to its collateral ligaments and the lateral meniscus intimately related to the structures of the posterolateral corner. (The illustration shows the structures of the right knee from the front. LCL=lateral collateral ligament, MCL=medial collateral ligament).
The posterolateral corner has a complex anatomy that is often poorly understood by orthopaedic surgeons, but an understanding of its anatomy and contribution to knee stability is essential if one is to avoid many of the problems of failed cruciate ligament surgery.
References
1 Noyes FR, Barber-Westin SD: Anterior cruciate ligament revision reconstruction: Results using a quadriceps tendon-patellar bone autograft. Am J Sports Med 34: 553-564, 2006.
2 Noyes FR and Barber-Westin SD: Revision anterior cruciate ligament reconstruction: Report of 11-year experience and results in 114 consecutive patients. In Instructional Course Lectures, Vol. 50, Sim FH (ed), American Academy of Orthopaedic Surgeons, Rosemont, IL, 2001, pp. 451-461.
3 Noyes FR and Barber-Westin SD: Revision anterior cruciate ligament surgery with use of bone-patellar tendon-bone autogenous grafts. J. Bone Joint Surg. 83-A: 1131-1143, 2001.
4 Noyes FR and Barber-Westin SD: Revision anterior cruciate ligament surgery with allograft and autograft tissues: Experience from Cincinnati. Clin Orthop 325: 116-129, 1996.
5 Noyes FR, Barber-Westin SD, and Roberts CS: Use of allografts after failed treatment of rupture of the anterior cruciate ligament. J Bone Joint Surg 76-A: 1019-1031, 1994.
6 Noyes FR, Barber-Westin SD: Posterior cruciate ligament revision reconstruction, part 1: Causes of surgical failure in 52 consecutive operations. Am J Sports Medicine 33: 646-654, 2005.
7 Noyes FR, Barber-Westin SD: Posterior cruciate ligament revision reconstruction, part 2: Results of revision using a two-strand quadriceps tendon-patellar bone autograft. Am J Sports Medicine 33: 655-665, 2005.
8 Noyes FR, Barber-Westin SD, Albright JC: An analysis of the causes of failure in 57 consecutive posterolateral operative procedures. Am J Sports Med 34: 1419-1430, 2006.
INTRODUCTION: ACL reconstruction failure and revisions