Revision from trans-tibial to 'more anatomic'
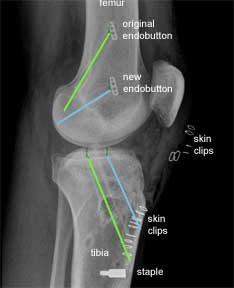
This is an X-ray of a patient who had a trans-tibial ACL reconstruction performed in another hospital. This was revised to a ‘more anatomic’ single bundle ACL, when it failed. The old femoral tunnel is highlighted in green and the new femoral tunnel is highlighted in blue.

This X-ray is from the front as before. The original endobutton was not removed. If you follow the line of the new femoral tunnel it is clear that it has been drilled from an antero- medial portal as the blue line points to two skin clips at this point.
There are further skin clips indicating an antero-lateral arthroscopic portal and a medial proximal tibial incision made to harvest the hamstring graft and drill the tibial tunnel. The larger white implant at the lower end of the tibia is a staple. This is put in for extra support in revision cases. This is in addition to the PEEK screw which was described earlier.
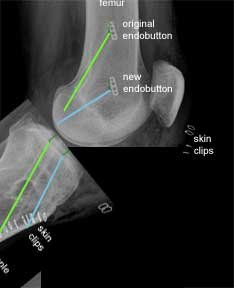
This is an X-ray, of the same patient, taken from the side instead of the front. The green lines show the original tunnels and the blue lines the new tunnels.
For the femoral tunnels the higher endobutton is from the original procedure and the lower endobutton is from the revision procedure.
The new tibial tunnel (blue) is more anterior (closer to the front) than the original tunnel. This is a more anatomic position for the tibial insertion of the native ACL.
To further help you to appreciate the differences between the two procedures, I have used a software programme to 'bend' the knee in the X-ray. This shows that the older trans-tibial procedure leads to parallel femoral and tibial tunnels. This is in contrast to the angled tunnels achieved using the ‘more anatomic’ approach.
I hope this makes it easier for you to look at your own X-rays and understand which of the two techniques you have had. If your surgery was more than five years ago it is almost certain that it would have been a trans-tibial reconstruction. Many Surgeons are now embracing the concept of the ‘more anatomic’ placement of the femoral and tibial tunnels as the quest for better rotational stability and more normal knee kinematics continues.


