Repositioning of the tibial tubercle
The very first recorded operation for patellar pain or instability was described by César Roux in the late 19th century. His operation was we would call today a 'distal' re-alignment, i.e. a re-alignment operation that takes place distal to the kneecap. Specifically, this means moving the patellar tendon, and this is most commonly done by moving the tibial tuberosity (the part of the shin bone to which the tendon attaches).
Like all patellar procedures, tibial tuberosity transfers have each had their day in the sun. Maquet in Belgium described a transfer of the tibial tuberosity in the anterior direction. This made the tuberosity more prominent, i.e. it would stick out. This was designed to take pressure off the kneecap and therefore diminish pain.
Tibial tuberosity transfers (Maquet, Elmslie-Trillat, Fulkerson)
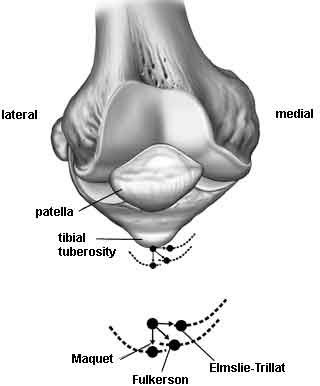
Elmslie in England and Trillat in France described moving the tibial tuberosity medially (towards the inside), a variation of Roux's procedure. This diminished the tendency of a patella to slide laterally (to the outside). Cox popularized the operation in the United States.
[Image reprinted with permission, The Adult Knee, Chapters 59-60, Lippincott Williams & Wilkins, 2003.]
Fulkerson in the United States combined these two transfers by slanting the bony cut of the tuberosity. The result is a displacement that is half way between a Maquet and an Elmslie-Trillat. There is some anterior displacement and some medial displacement. The specific slant of the cut determines whether there will be more anterior or medial displacement.
The indications for each of these tibial tuberosity transfer procedures are very much in the eye of the beholder.
None of these operations is magical.The only absolute is that a lateral retinacular release is indicated only when the lateral retinaculum is overly tight.
The distal re-alignments diminish the Q angle when they move the tt medially. The Maquet doesn't affect the Q angle, and the proximal re-alignment give the appearance of increasing the Q angle, since the patella moves medially. This is a question that often comes up at meetings. I answer by saying that the true Q angle is unmasked when the patella is centered.
