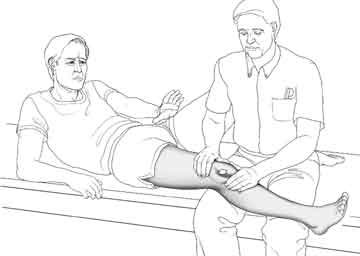
Supine (lying on one's back)
In this position the clinician can examine -
[All illustrations on this page are reprinted with permission, The Adult Knee, Chapters 59-60, Lippincott Williams & Wilkins, 2003.]
It is present in only the most severe forms of instability and, as such, is not a good screening test for patellar malalignment or even instability. However, when it is positive it usually indicates a serious anatomic variation or injury that will probably require surgery.
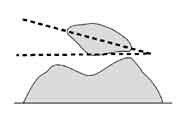

- patellar tilt - The normal kneecap lies flat. In other words, an imaginary line drawn between the borders of your kneecap should be parallel to the floor. In some patients the kneecap is tilted instead, like a beret. This is a form of so-called malalignment. A subset of such patients will have pain as a result of this malposition.
- tenderness under the patella - Patients with painful malalignment commonly exhibit tenderness about the patella. If the patella is tilted but not tender, the doctor should look elsewhere for a source of pain - it's not the patella.
- q-angle - At this point, the 'quadriceps' (Q) angle can be assessed. This somewhat complex angle starts way up at the hip and goes just past the knee. It reflects the relationship of various muscles and tendons about the kneecap and is one measure of how likely the kneecap is to be pushed off to the side. The normal is 15-20 degrees. When the Q angle is elevated (20 degrees or more) this represents another form of malalignment.
A common error among health professionals is to assume that the Q angle is the angle between the femur and tibia.
Although it is GENERALLY true that higher fem-tib. angles lead to higher Q angles and that lower fem-tib. angles lead to lower Q angles, it is not always true -which is why the lower limb of the Q angle is the a funny line from the center of the patella to the tibial tubercle, and not simply the axis of the tibia.
There exist a number of patients with tibia vara - the exact opposite of a knock-knee - and a large Q angle. This is because their tibial tubercle is quite lateralized.
I usually state that normal is 15-20 degrees, mainly because these are round numbers. I don't think you can be accurate within a degree with standard measuring tools.
High Q angles are bad, but low angles lead to fem-tib. arthritis [the downside to medializing the tibial tubercle on everyone], so we can't say that the lower the better. There's a healthy range.
